Malaria notes
- related: ID
This patient with recent travel to Sub-Saharan Africa has an acute-onset febrile illness, scleral icterus, mild splenomegaly, anemia, and thrombocytopenia. This presentation is most consistent with malaria.
Plasmodium falciparum accounts for the majority of deaths from malaria, followed by Plasmodium vivax. Many of the clinical symptoms seen in malaria are due to the infected parasite-containing red blood cells adhering to nearby vessels, causing small infarcts, leakage of capillaries, and, ultimately, organ dysfunction. Diagnosis is confirmed with examination of a peripheral blood smear looking for trophozoites.
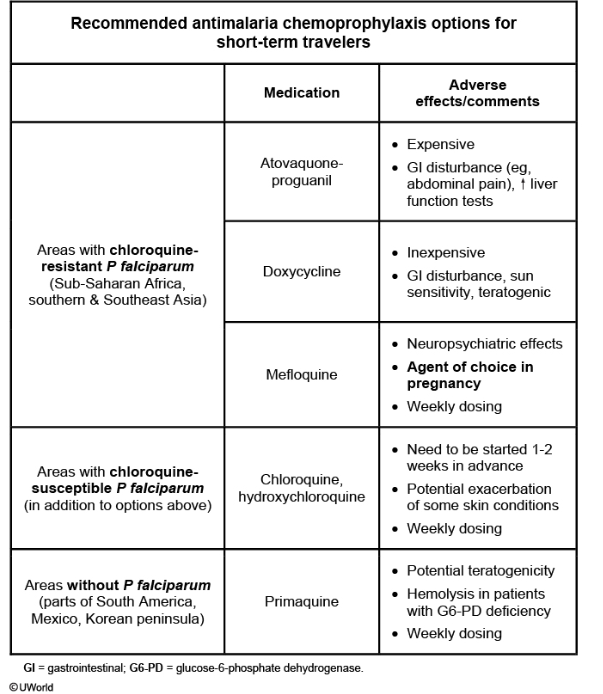
Commonly used malaria prophylaxis drugs (eg, chloroquine, mefloquine, and doxycycline) target the blood stage of the parasite (blood schizonticides) when released from the liver. Tissue schizonticides (eg, atovaquone/proguanil) are designed to target the liver stage, where the parasites grow and can stay dormant in the liver (or other tissues). The blood schizonticides must be continued for at least 4 weeks after leaving an endemic area to ensure eradication of parasites released from the liver.
This patient did take doxycycline for malaria prophylaxis but discontinued his medication on return to the United States, causing it to be ineffective.